Spondylosis is age-related wear and tear of the spine that affects the discs, joints and vertebrae. It commonly occurs in the neck (cervical spondylosis) or lower back (lumbar spondylosis), causing pain, stiffness and sometimes nerve symptoms.
Rather than a single disease, spondylosis acts as an umbrella term encompassing several spine conditions, such as:
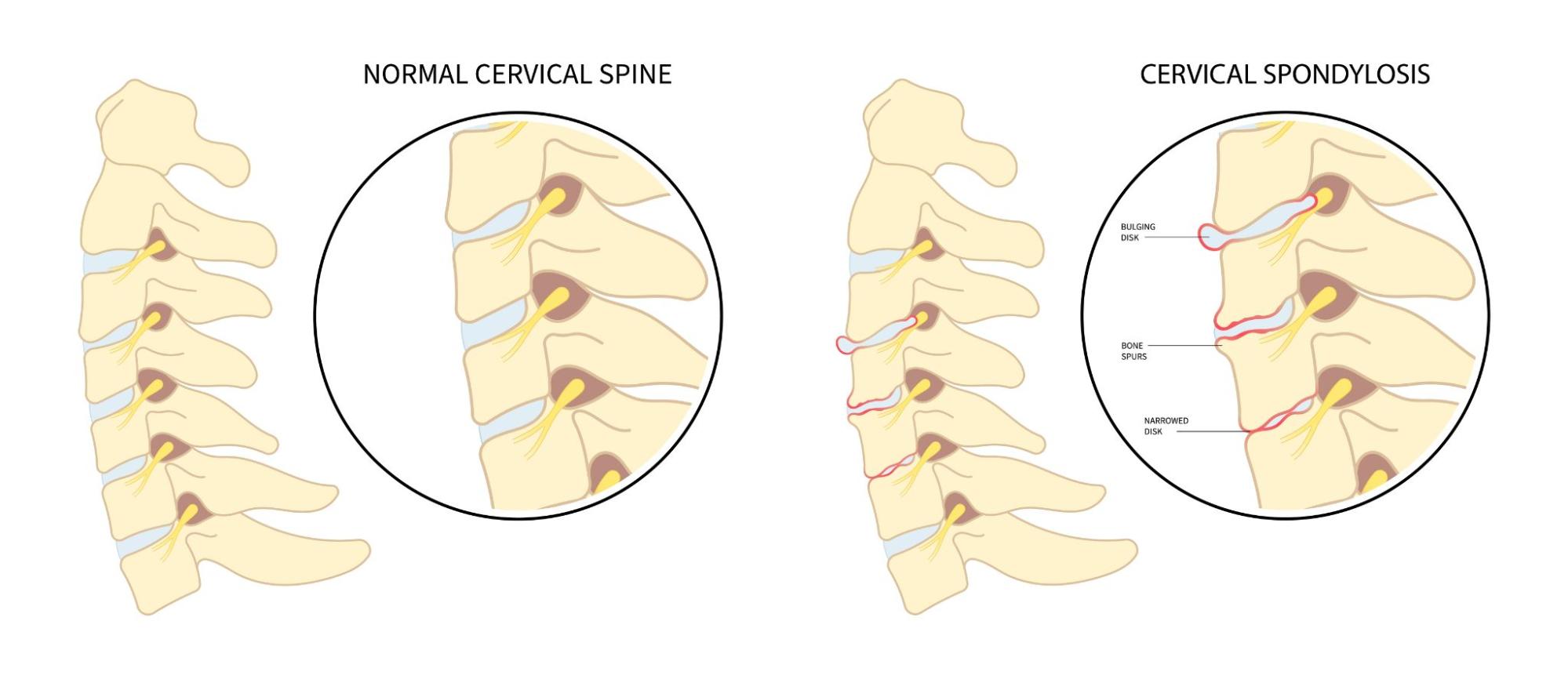
Although spondylosis acts as an umbrella term encompassing several spine-related conditions, this page focuses specifically on degenerative spinal changes caused by gradual wear and tear.
The condition develops gradually due to cumulative mechanical stress and the biological ageing process within the spine. This can include:

Symptoms vary depending on the affected spinal region and the degree of nerve involvement. Although many individuals remain asymptomatic despite imaging findings, the symptoms may present themselves as:
Spondylosis is often caused by degenerative changes leading to disorders of the spine. However, certain factors increase its susceptibility, such as:
Diagnosing spondylosis involves a careful combination of clinical assessment and imaging studies. This is to confirm degenerative changes in the spine and determine whether nerves or the surrounding structures are affected.
The process generally involves:


The treatment of spondylosis focuses on relieving pain, reducing nerve irritation and maintaining spinal function. It is tailored to the severity of the symptoms, the specific spinal structures involved and how much daily activity is affected.
This may involve:

Spondylosis describes age- and wear-related changes in the spine that can gradually lead to pain, stiffness or nerve irritation. While it is more common as we grow older, it can also affect younger adults following injuries, long hours of strain or repeated stress on the spine. Symptoms may start subtly and worsen over time, often interfering with daily comfort, mobility and sleep if left unaddressed.
If back or neck pain has been holding you back, speaking to a doctor early can make a real difference in regaining comfort and confidence in everyday movement.
Spondylosis is linked to natural wear and tear of the spine, so it cannot be reversed entirely. However, this does not mean you have to live with ongoing discomfort. With the right combination of medical care, physiotherapy and lifestyle adjustments, symptoms can often be well controlled and quality of life significantly improved. In more advanced cases, targeted procedures or surgery may be considered to relieve pressure on nerves and restore function.
While ageing cannot be prevented, maintaining good posture, staying physically active and strengthening the core and back muscles can help reduce strain on the spine. Using proper technique during exercise, avoiding prolonged sitting and managing body weight also support long-term spinal health and may slow degenerative changes.
If neck or lower back pain persists for several weeks, keeps returning or begins to interfere with daily activities, it is advisable to seek medical assessment. Symptoms such as numbness, tingling, weakness in the arms or legs, or difficulty walking should be evaluated promptly, as early care often leads to better outcomes.
Spondylosis is a broad term that describes degenerative changes in the spine. These changes can contribute to conditions such as slipped discs or spinal stenosis, but they are not identical. A proper assessment helps identify which structures are involved and guides the most appropriate treatment plan.
Yes. Physiotherapy plays an important role in managing spondylosis by improving spinal mobility, strengthening supportive muscles and reducing pain. Many people find that regular, guided exercise helps them move more comfortably and stay active over the long term.
In some individuals, symptoms may remain stable, while in others they can gradually worsen over time. Without treatment, pain, stiffness or nerve-related symptoms may become more persistent. Early evaluation and personalised care can help slow progression and prevent unnecessary limitations.
No. Most people with spondylosis improve with non-surgical treatments such as medication, physiotherapy and targeted injections. Surgery is usually reserved for cases where symptoms are severe, progressive or do not respond to conservative care.
Dr Wilson Tay is skilled in ultrasound-guided pain interventions that provide safer, more precise relief without unnecessary radiation exposure. His expertise covers a wide range of conditions including spine pain, headaches, abdominal and pelvic pain, fibromyalgia and cancer pain.


MMed (Anaes) | FIPP (World Institute of Pain, USA) | FAMS (Anaes) | Grad Dip Acupuncture (Singapore)
Consultant Pain Specialist, Consultant Anaesthesiologist, Registered Acupuncturist MBBS
Dr Wilson Tay is skilled in ultrasound-guided pain interventions that provide safer, more precise relief without unnecessary radiation exposure. His expertise covers a wide range of conditions including spine pain, headaches, abdominal and pelvic pain, fibromyalgia and cancer pain.


